


 Sign Out
Sign Out

Dosage: Breast cancer: Combination Therapy: When used in combination therapy with docetaxel for the treatment of metastatic breast cancer in patients with disease that failed to respond to or recurred following anthracycline-containing chemotherapy, the recommended initial dosage of capecitabine is 1250 mg/m2 twice daily (morning and evening), equivalent to a total daily dose of 2500 mg/m2, for 2 weeks followed by a 1-week rest period; courses of therapy are given in 3-week cycles. Docetaxel 75 mg/m2 is administered as a 1-hour IV infusion on the first day of each 3-week cycle. Patients should be premedicated prior to docetaxel administration. Treatment with the combination regimen was continued for at least 6 weeks in the randomized trial.
Monotherapy: For the palliative treatment of metastatic breast cancer in patients with disease resistant to both paclitaxel and an anthracycline-containing chemotherapy regimen or in patients with disease resistant to paclitaxel who are not candidates for further anthracycline therapy, the recommended initial dosage of capecitabine is 1250 mg/m2 twice daily (morning and evening), equivalent to 2500 mg/m2 total daily dose, for 2 weeks followed by a 1-week rest period; courses of therapy are given in 3-week cycles.
Colorectal Cancer: Adjuvant Therapy for Colon Cancer: For adjuvant therapy following the complete resection of primary tumor in patients with stage III (Dukes' C) colon cancer when treatment with fluoropyrimidine therapy alone is preferred, the recommended dosage of capecitabine is 1250 mg/m2 twice daily (morning and evening) for 2 weeks followed by a 1-week rest period; courses of therapy are given in 3-week cycles for a total of 8 cycles and a treatment period of 6 months.
First-line Therapy for Metastatic Colorectal Cancer: For the first-line treatment of metastatic colorectal cancer when treatment with fluoropyrimidine therapy alone is preferred, the recommended initial dosage of capecitabine is 1250 mg/m2 twice daily (morning and evening), equivalent to 2500 mg/m2 total daily dose, for 2 weeks followed by a 1-week rest period; courses of therapy are given in 3-week cycles.
Dosage Calculation: Round to the nearest dose that gives a whole tablet rather than cutting tablets in half. (See Table 1.)
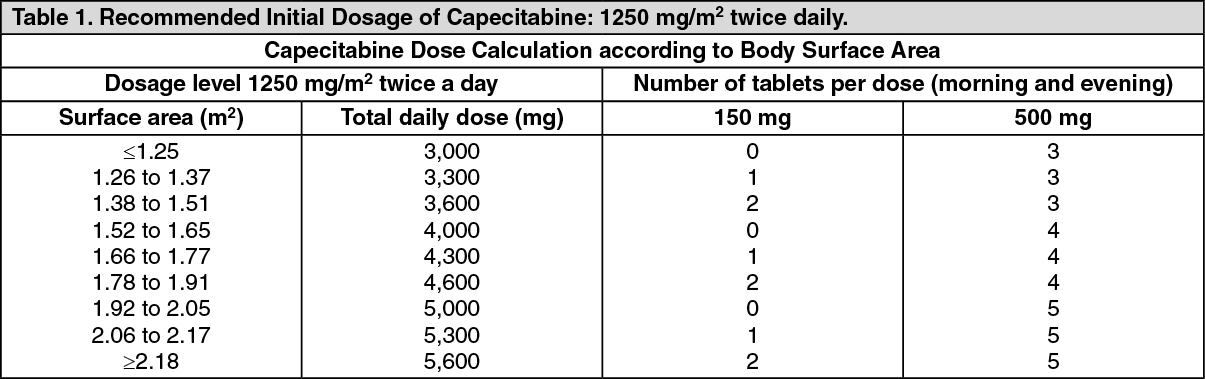 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDosage modification for Age-related Effects: Some clinicians recommend that capecitabine dosage be reduced (eg; initial dosage reduced by up to 20%) in patients older than 80 years of age receiving capecitabine monotherapy. Because of decreased tolerance of the combination regimen of capecitabine and docetaxel for advanced breast cancer in patients 60 years of age or older, a 25% reduction of the initial capecitabine dose (to 950 mg/m2) should be considered.
Dosage Modification for Toxicity: After the initial dose of capecitabine, subsequent doses should be modified as necessary based on individual patient tolerance with careful monitoring to obtain optimal therapeutic response with minimal toxicity. The dose-limiting toxicities of capecitabine include diarrhea, nausea, vomiting, abdominal pain, palmar-plantar erythrodysesthesia (hand-foot syndrome), and leukopenia.
If a patient experience a grade 4 toxicity, the drug should be discontinued or therapy interrupted until the toxicity resolves or decreases in intensity to grade 1; if capecitabine therapy is resumed, the dose should be decreased to 50% of the original dose. If a patient experiences a grade 2 or 3 toxicity, capecitabine therapy should be interrupted until the toxicity resolves or decreases in severity to grade 1.
At the start of the next treatment cycle, subsequent doses should be reduced according to the severity and recurrence of the toxicity as shown in the following table on Recommended Dosage Modifications for Toxicity of Capecitabine Monotherapy. The manufacturer states that once the capecitabine dosage has been reduced, the dosage should not be increased at a later time.
When capecitabine therapy is interrupted because of toxicity, therapy should be resumed according to planned treatment cycles; doses of the drug omitted because of toxicity should not be replaced. (See Table 2 and 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image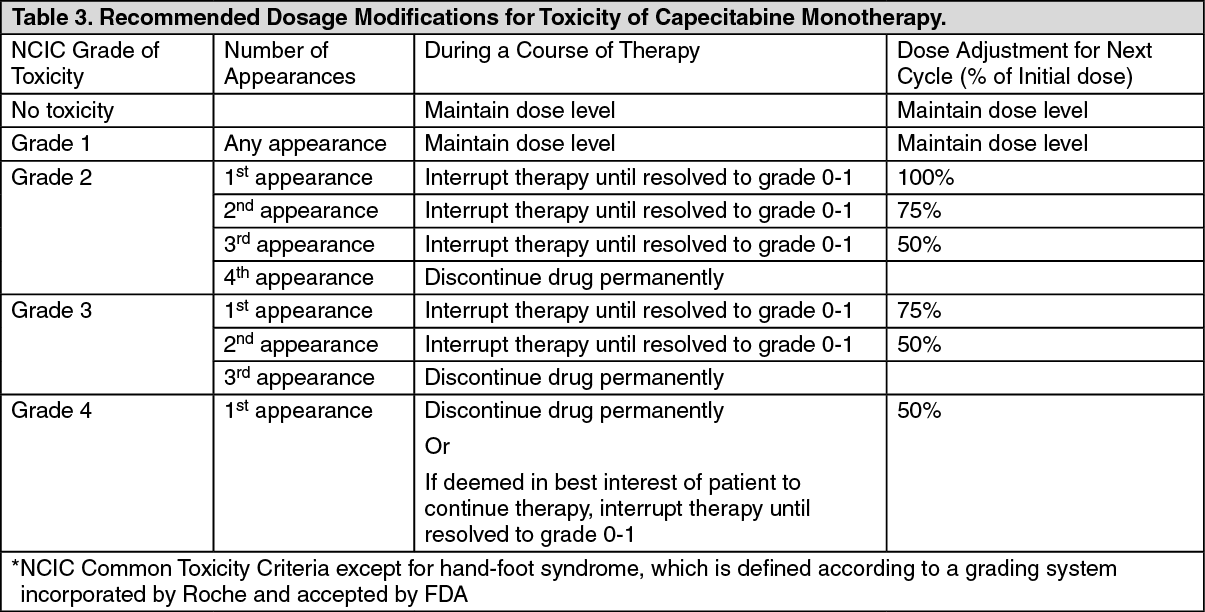 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAll dose modifications should be based on the worst preceding toxicity.
Dosage in Renal and Hepatic Impairment: Capecitabine is contraindication in patients severe renal impairment (i.e; creatinine clearance less than 30 mL/minute calculated with the formula of Cockcroft-Gault). In patients with moderate renal impairment (i.e creatinine clearance 30-50 mL/minute calculated with the formula of Cockcroft-Gault), a dosage reduction to 75% of the initial capecitabine dose when used as monotherapy or in combination with docetaxel (i.e; from 1250 to 950 mg/m2 twice daily) is recommended. No adjustment in starting dose is recommended in patients with mild renal impairment. Careful monitoring is required in patients with mild or moderate renal impairment receiving capecitabine because the frequency and/or severity of adverse effects of capecitabine may be increased. If the patient develops a grade 2, 3, or 4 adverse effect, treatment with capecitabine should be discontinued promptly, and subsequent dose modification for toxicity should be made.
The effects of hepatic impairment on the pharmacokinetics of capecitabine have not been fully evaluated. The manufacturer states that no adjustment in initial dosage of capecitabine is necessary in patients with mild to moderate hepatic dysfunction secondary to liver metastases. However, caution is advised and patients with mild to moderate hepatic dysfunction should be monitored carefully during capecitabine therapy. The safety and efficacy of capecitabine in patients with severe hepatic impairment have not been evaluated.
Paediatric population: There is no experience in children (under 18 years).